Coffee Boosts Stroke Risk, Study Finds
by Allison Gandey
November 5, 2010 — A cup of coffee can heighten the risk for ischemic stroke, particularly among infrequent drinkers, report researchers. Their study provides new information that may be useful in stroke prevention and is in line with what is already known about the physiologic effects of coffee.
Investigators led by Elizabeth Mostofsky, MPH, from Harvard Medical School in Boston, Massachusetts, found a 2-fold increased stroke risk in the hour after drinking a cup of coffee. The increased risk returned to baseline within a 2-hour window, which investigators say strengthens the possibility of a causal relationship.
The work appears in the November 2 issue ofNeurology.
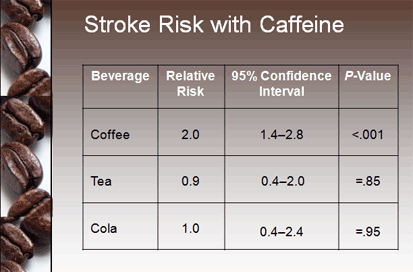 |
| The risk was highest in the hour after drinking coffee. |
Previous studies evaluating the effect of coffee on cardiovascular diseases have provided conflicting results. Case-control studies have shown an increase in risk, but prospective cohort studies have suggested no harmful effects. Coffee has been shown to have a negative effect on cardiovascular biomarkers increasing serum cholesterol, insulin resistance, and plasma homocysteine. However, several studies have shown that coffee intake decreases the risk for type 2 diabetes.
In this new multicenter crossover study, researchers interviewed 390 people with ischemic stroke. They compared each person's coffee intake the hour before stroke symptoms to his or her usual consumption.
Most people, 78%, said they drank coffee the prior year. More than half of these had a cup of coffee within 24 hours of stroke. Close to 9% of patients had coffee within 1 hour of stroke onset.
Although an increase in stroke risk was seen with coffee, there was no apparent increase in risk in the hour after a cup of caffeinated tea or cola.
The association between ischemic stroke in the hour after coffee consumption was only apparent among those consuming 1 cup or less per day and not for those who drank coffee more regularly (P for trend = .002). Relative risks remained similar when researchers restricted the sample to those who were not simultaneously exposed to other potential triggers, and the results remained significant after stratifying by time of day.
"Elegant Study Design"
In an accompanying editorial, Giancarlo Logroscino, MD, from University of Bari in Italy, and Tobias Kurth, MD, from the Institut National de la Santé et de la Recherche Médicale in Paris, France, say "the authors used an elegant study design" and they call this "an important addition to the 'coffee paradox'."
But they add clinicians will need further evidence to properly advise people about coffee intake, especially when other risk factors for stroke are present.
"Even if coffee contains other substances that may be responsible for the observed effect, caffeine is the most likely candidate for pulling the trigger," they note.
The peak plasma concentration of caffeine is usually less than 2 hours and has several systemic effects, including rapidly increasing epinephrine release, blood pressure, and insulin sensitivity, they explain. "Caffeine has both systemic and cerebral vasoconstrictive effects."
Lead study author Elizabeth Mostofsky reports receiving research funds from the National Institutes of Health and the National Institute of Allergy and Infectious Diseases. Editorialist Giancarlo Logroscino has received research support from the Amyotrophic Lateral Sclerosis Association, the Italian Ministry of Health, the University of Bari, the Apulia Region, and the Italian Ministry of University. Dr. Logroscino has also received compensation for services from Pfizer, Novartis, GlaxoSmithKline, and Eli Lilly. Dr. Tobias Kurth has received support from the National Institutes of Health, the French National Research Agency, the Migraine Research Foundation, and the Parkinson's Disease Foundation. He serves as a consultant for i3 Drug Safety and World Health Information Science Consultants. He has also received funding from Genzyme, Merck Serono, and Pfizer.
Neurology. 2010;75:1583-1588.
No comments:
Post a Comment