Friday, November 19, 2010
Thursday, November 18, 2010
Senate & House Unveil Possible Temporary Fix for Medicare
by Robert Lowes
November 18, 2010 — House Democrats introduced legislation today that would postpone a 23% cut in Medicare reimbursement for physicians set for December 1 until January 1, 2012, and instead boost rates by 1% in the meantime.
Meanwhile, Sen. Max Baucus (D-MT), the chair of the Senate Finance Committee, and Sen. Chuck Grassley (R-IA), the committee’s ranking Republican member, unveiled a 2-part plan that also would spare physicians the massive pay cut for 13 months.
Under the senators’ bipartisan agreement, the Senate would delay the December 1 pay cut until January 1, and in the meantime craft another extension for the rest of 2011. The 1-month delay would be paid for with savings achieved elsewhere in the Medicare program. The financing for the longer extension has yet to be worked out.
The House was scheduled to adjourn this afternoon for the Thanksgiving holiday and return on November 29. The Senate’s timetable for adjournment this week is still up in the air. If the 2 chambers of Congress fail to pass and reconcile their respective Medicare “doc fix” plans this week, they still have November 29 and November 30 to finish up.
Brendan Daly, a spokesperson for House Speaker Nancy Pelosi (D-CA), told Medscape Medical News that the House would consider the 1-month Senate extension on November 29. The timing on the 13-month House bill has yet to be determined, Daly said.
Organized medicine has warned that if the 23% pay cut takes effect, many physicians will close their doors to new Medicare patients and even drop out of the federal program. To make matters worse, another Medicare cut of roughly 2% is scheduled for January 1.
Bipartisan Lip Service for Permanent Fix, Clash Over Financing
Organized medicine, along with the Obama administration, supports delaying the Medicare pay cut until 2012 — the so-called 13-month fix — as a way to buy Congress more time to devise a permanent solution to the Medicare reimbursement crisis. At its heart is the sustainable growth rate (SGR) formula that Congress created in 1997 to help control Medicare spending. The formula sets a target for annual Medicare expenditures on physician services based partly on growth in the gross domestic product. If actual spending in 1 year tops the target, Medicare is supposed to reduce physician reimbursement the following year to recoup the difference.
The American Medical Association and other medical societies argue that the formula is defective because physician practice expenses grow at a faster pace than the gross domestic product. They support replacing the SGR formula with one more squarely based on the Medicare Economic Index, which measures inflation in physician practice costs.
The SGR formula has triggered pay cuts every year going back to 2003, but Congress has postponed each one. However, the difference between targeted and actual spending accumulates from year to year, meaning the cuts keep getting bigger.
The notion of a permanent doc fix attracts lip service from Democrats and Republicans alike. Where the 2 parties part ways is over how to foot the bill.
The Congressional Budget Office estimates that merely freezing current Medicare rates through 2020 as opposed to decreasing them would cost taxpayers $276 billion. Giving physicians raises based on the Medicare Economic Index ups the ante to $330 billion.
In the past, Congressional Democrats have been willing to pay for such ambitious payment reforms through deficit spending. Republicans, in contrast, have insisted on cutting the budget elsewhere to finance even the smallest of doc fixes. With Republicans now in charge of the House, the debate over financing will go up several notches, especially because lawmakers will be challenged to find hundreds of billions of dollars in the federal budget that they can excise to offset a permanent fix.
Thursday, November 11, 2010
A Fat Attack Can Kill You
 What is a "Fat Attack?" A "Fat Attack" is defined as a gain of more than 5% of your total body weight. A gain of this much weight can be notably detrimental to your health. Gaining just 5% of your total body weight increases your risk for diabetes, heart disease, hypertension, stroke, osteoarthritis, polycysitic ovarian disease, allergies, and the list goes on . . . Most importantly, your weight gain significantly affects your life and increases your risk of death by 20-40% according to recent study in the New England Journal of Medicine.
What is a "Fat Attack?" A "Fat Attack" is defined as a gain of more than 5% of your total body weight. A gain of this much weight can be notably detrimental to your health. Gaining just 5% of your total body weight increases your risk for diabetes, heart disease, hypertension, stroke, osteoarthritis, polycysitic ovarian disease, allergies, and the list goes on . . . Most importantly, your weight gain significantly affects your life and increases your risk of death by 20-40% according to recent study in the New England Journal of Medicine. Between 300,000-400,000 deaths occur every year due to obesity. 435,000 deaths occurred due to smoking in 2008 according to the CDC. Obesity is just as dangerous as smoking
"Overweight and obesity are now so common that they are replacing the more traditional public health concerns such as under-nutrition and infectious disease as some of the most significant contributors to ill health." (World Health Organization 1997 statement on obesity.)
So what should you do if you're having a "Fat Attack?" You should follow up with a your physician or a weight management specialist, a physician that is specialty trained in the treatment of obesity and its related disorders.
You can find a physician that has this special training through the American Society of Bariatric Physicians. These physicians have significant specialty training in identifying and successfully treating overweight and obesity conditions.
You can be successful in loosing weight and your "Fat Attack" shouldn't lead you to a heart attack. Look up your nearby bariatrician and start your treatment today.
Saturday, November 6, 2010
EHR Incentive Money is Taxable
CMS' EHR Meaningful Use Bonus Money Subject to Federal Taxes

(Taken from AAPF News)
By Sheri Porter
10/20/2010
10/20/2010
Are CMS incentive payments, which are available to physicians who invest in electronic health records, or EHRs, and use them in a meaningful way, taxable by the IRS? That question was asked during the recent AAFP Town Hall meeting in Denver.
The simple answer is "yes." According to Steven Waldren, M.D., director of the AAFP's Center for Health IT, all health IT incentive payments received as a part of the American Recovery and Reinvestment Act of 2009 and the accompanying Health Information Technology for Economic and Clinical Health, or HITECH, Act are viewed by the IRS as taxable income.
Physicians who meet the incentive payment criteria are eligible to earn as much as $44,000 from Medicare, or they can choose to earn Medicaid incentives of as much as $63,750.
Waldren, who consulted with the Office of the National Coordinator for Health IT, noted that family physicians should consult their tax accountants for recommendations on how to manage the tax burden.
Physicians who meet the incentive payment criteria are eligible to earn as much as $44,000 from Medicare, or they can choose to earn Medicaid incentives of as much as $63,750.
Waldren, who consulted with the Office of the National Coordinator for Health IT, noted that family physicians should consult their tax accountants for recommendations on how to manage the tax burden.
TIPS FROM A TAX EXPERT
Mark Estroff, C.P.A., a principal at Gates Moore and Co., an Atlanta-based health care consulting and accounting firm, explained how the government is viewing the incentive program.
"The way I look at it, this is just enhanced reimbursement from the federal program," he told AAFP News Now. "They're just going to give you a little more money because you're utilizing the proper technology in your practice, and it is taxable just like any other practice gross receipts that you're going to receive."
Estroff added that there are some tax advantages for medical practices. For example, when physicians buy equipment -- whether it's hardware or most software -- the IRS allows them to write off as much as 100 percent of the cost of that equipment. However, that write-off is subject to the limitations of the optional expensing rules of Internal Revenue Code Section 179, Estroff added.
"Depending on how you go about it -- the tax law limitations, the size of your practice and a lot of other factors -- you may be able to write it all off in the year that you acquire it," he said, although in other situations, it may take five years to recover the investment through tax benefits.
Estroff also advised physicians to comb their state tax laws to see if there are additional tax incentives -- as is the case in Georgia -- for upgrading their practice technology or for training staff to use a health IT system.
Putting himself in the role of a qualifying physician, "it's another cash infusion into my practice to help me pay for the cost of the EHR," said Estroff.
"The way I look at it, this is just enhanced reimbursement from the federal program," he told AAFP News Now. "They're just going to give you a little more money because you're utilizing the proper technology in your practice, and it is taxable just like any other practice gross receipts that you're going to receive."
Estroff added that there are some tax advantages for medical practices. For example, when physicians buy equipment -- whether it's hardware or most software -- the IRS allows them to write off as much as 100 percent of the cost of that equipment. However, that write-off is subject to the limitations of the optional expensing rules of Internal Revenue Code Section 179, Estroff added.
"Depending on how you go about it -- the tax law limitations, the size of your practice and a lot of other factors -- you may be able to write it all off in the year that you acquire it," he said, although in other situations, it may take five years to recover the investment through tax benefits.
Estroff also advised physicians to comb their state tax laws to see if there are additional tax incentives -- as is the case in Georgia -- for upgrading their practice technology or for training staff to use a health IT system.
Putting himself in the role of a qualifying physician, "it's another cash infusion into my practice to help me pay for the cost of the EHR," said Estroff.
TAKE ADVANTAGE OF INCENTIVES
Estroff makes sure that his physician and health care professional clients are aware that the HITECH incentive offer is a once-in-a-lifetime chance to boost their income.
"If they do not implement (an EHR) and take advantage of this extra money that's being offered, eventually they're going to be penalized," said Estroff. The federal program offers several years of bonus payments, but in 2015, CMS will begin penalizing physicians who aren't using EHRs by reducing their Medicare payments.
"Right now, physicians are getting the carrot before the stick," said Estroff. "They're going to get the stick in a few years, so they might as well eat the carrot while they can."
Estroff concluded with this tip: "The tax question is a basic question. The real issue goes back to selecting the right (EHR) product," and that means physicians have to take a hard look at their practices' needs and capabilities. "There's a whole selection process that takes place, and you don't often let the tax implications drive your decision," said Estroff.
"If they do not implement (an EHR) and take advantage of this extra money that's being offered, eventually they're going to be penalized," said Estroff. The federal program offers several years of bonus payments, but in 2015, CMS will begin penalizing physicians who aren't using EHRs by reducing their Medicare payments.
"Right now, physicians are getting the carrot before the stick," said Estroff. "They're going to get the stick in a few years, so they might as well eat the carrot while they can."
Estroff concluded with this tip: "The tax question is a basic question. The real issue goes back to selecting the right (EHR) product," and that means physicians have to take a hard look at their practices' needs and capabilities. "There's a whole selection process that takes place, and you don't often let the tax implications drive your decision," said Estroff.
It's the Coffee, Not the Caffeine . . .
Coffee Boosts Stroke Risk, Study Finds
by Allison Gandey
November 5, 2010 — A cup of coffee can heighten the risk for ischemic stroke, particularly among infrequent drinkers, report researchers. Their study provides new information that may be useful in stroke prevention and is in line with what is already known about the physiologic effects of coffee.
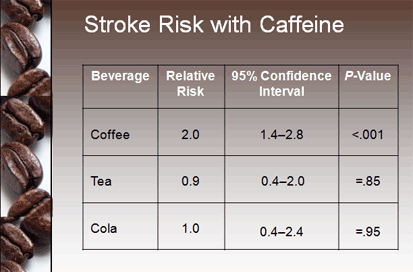
Investigators led by Elizabeth Mostofsky, MPH, from Harvard Medical School in Boston, Massachusetts, found a 2-fold increased stroke risk in the hour after drinking a cup of coffee. The increased risk returned to baseline within a 2-hour window, which investigators say strengthens the possibility of a causal relationship.
The work appears in the November 2 issue ofNeurology.
 |
| The risk was highest in the hour after drinking coffee. |
Previous studies evaluating the effect of coffee on cardiovascular diseases have provided conflicting results. Case-control studies have shown an increase in risk, but prospective cohort studies have suggested no harmful effects. Coffee has been shown to have a negative effect on cardiovascular biomarkers increasing serum cholesterol, insulin resistance, and plasma homocysteine. However, several studies have shown that coffee intake decreases the risk for type 2 diabetes.
In this new multicenter crossover study, researchers interviewed 390 people with ischemic stroke. They compared each person's coffee intake the hour before stroke symptoms to his or her usual consumption.
Most people, 78%, said they drank coffee the prior year. More than half of these had a cup of coffee within 24 hours of stroke. Close to 9% of patients had coffee within 1 hour of stroke onset.
Although an increase in stroke risk was seen with coffee, there was no apparent increase in risk in the hour after a cup of caffeinated tea or cola.
The association between ischemic stroke in the hour after coffee consumption was only apparent among those consuming 1 cup or less per day and not for those who drank coffee more regularly (P for trend = .002). Relative risks remained similar when researchers restricted the sample to those who were not simultaneously exposed to other potential triggers, and the results remained significant after stratifying by time of day.
"Elegant Study Design"
In an accompanying editorial, Giancarlo Logroscino, MD, from University of Bari in Italy, and Tobias Kurth, MD, from the Institut National de la Santé et de la Recherche Médicale in Paris, France, say "the authors used an elegant study design" and they call this "an important addition to the 'coffee paradox'."
But they add clinicians will need further evidence to properly advise people about coffee intake, especially when other risk factors for stroke are present.
"Even if coffee contains other substances that may be responsible for the observed effect, caffeine is the most likely candidate for pulling the trigger," they note.
The peak plasma concentration of caffeine is usually less than 2 hours and has several systemic effects, including rapidly increasing epinephrine release, blood pressure, and insulin sensitivity, they explain. "Caffeine has both systemic and cerebral vasoconstrictive effects."
Lead study author Elizabeth Mostofsky reports receiving research funds from the National Institutes of Health and the National Institute of Allergy and Infectious Diseases. Editorialist Giancarlo Logroscino has received research support from the Amyotrophic Lateral Sclerosis Association, the Italian Ministry of Health, the University of Bari, the Apulia Region, and the Italian Ministry of University. Dr. Logroscino has also received compensation for services from Pfizer, Novartis, GlaxoSmithKline, and Eli Lilly. Dr. Tobias Kurth has received support from the National Institutes of Health, the French National Research Agency, the Migraine Research Foundation, and the Parkinson's Disease Foundation. He serves as a consultant for i3 Drug Safety and World Health Information Science Consultants. He has also received funding from Genzyme, Merck Serono, and Pfizer.
Neurology. 2010;75:1583-1588.
Monday, November 1, 2010
My Electronic Medical Record Reality
 I love my electronic medical record (EMR). I can type about 100-110 words a minute, but I just installed Dragon Medical. It is amazing. I can now dictate 600 words per minute. My day just sped up and I might make it home for dinner!
I love my electronic medical record (EMR). I can type about 100-110 words a minute, but I just installed Dragon Medical. It is amazing. I can now dictate 600 words per minute. My day just sped up and I might make it home for dinner! Those of you that know me know that I have been using an EMR since 2002 when I opened my practice. Many people I spoke to told me I was "nuts" to consider practicing Solo. When I told them I had purchased and EMR they would roll their eyes and moan.
Those of you that know me know that I have been using an EMR since 2002 when I opened my practice. Many people I spoke to told me I was "nuts" to consider practicing Solo. When I told them I had purchased and EMR they would roll their eyes and moan. Times have changed slightly. Recent data states that 36-41% of physicians are using at least a partial EMR/EHR this year. That's up from 17% just two years ago. Much of this change is due to the government mandate to adopt electronic health records (EHRs) by 2014.
So, why am I a fan? Yes, it feels like another government push to monitor our actions and control our decisions. And yes, they changed the acronym, too. But, I think there are some benefits to be had with these changes. Before congress ever got their fingers on it, I realized that EHRs could offer me five areas of freedom.
Automation:
In medical school and residency I found that I was often rewriting the same information over and over and over . . . . "Cardiovascular exam reveals heart with a regular rate and rhythm without murmur. No lifts or thrills. . . " And one day I thought, "That's true, there are no 'lifts or thrills' to writing this again and again." I found that in most cases I was re-writing much of the same information multiple times each day with only a few differences between patient exams. I remembered some basic programing skills I picked up in junior high school demonstrated then that I could get a computer to write the same things repeatedly a whole lot faster than I could write them with my black pen (and it would be legible, too).
Efficiency:
I knew that my home computer could calculate my checkbook for me, and my telephone could store all my contacts at my fingertips. Why couldn't my office computer make my writing of chart notes easier, more legible, and then transmit that data to a pharmacy or to a lab? Why couldn't I have all my laboratory data in on place that I could compare and trend?
I realized two very important things. First, doing today's work today (and actually finishing it) seemed to make me feel better at the end of the day. Second, I spent 13 years of my life and thousands of educational dollars learning to make difficult life-or-death decisions. If what I am really being paid to do is make important decisions, then why am I doing all the other stuff that takes up all the time in my day? I found that on days I made decisions more efficiently and finished all of the day's work today, I felt much happier. The sky seemed "bluer."
 Mobility:
Mobility:I can't tell you how many times I have been at the grocery store or at the restaurant and a patient would call with a question about a lab or an x-ray or a medication that my Physician Assistant had written that I knew nothing about. Isn't there some way I could use the same phone that I carry around everywhere with me to check these things? I could use my phone in real time to check stocks, my bank account, and see the dress made of steaks Lady Gaga is wearing. Why can't I check my charts? Well, now, I can, and I do. I use Remote Desktop for Android by Xtralogic. Once in a while, now, I can enjoy the blue sky.
Legibility:
My handwriting looks like chicken scratch, especially after a long day. The busier the day, the more hen pecked it looks. I found that I can type or dictate much faster than I can legibly write. Why am I still writing in paper charts? I'm not. My nurse transcribes the first part of my note in the room for me while I do my examination. Then, between patients, I put the finishing touches on my note with Nuance's Dragon Medical voice recognition dictation software that works seamlessly with my EMR.
Writer's Cramp:
With an electronic medical record I no longer get writer's cramp. My third finger no longer has that painful callous; now I just have to avoid carpal tunnel.
Retrieve Data, Understand Data, Make Your Decision:
I remember as a medical student some great wisdom from on of my supervising residents. He stated that we were trained to make decisions, and any tool that would help you rapidly retrieve the data, rapidly understand that data, and then make relevant decisions based on that data was well worth its cost. Well, I found that is exactly what the EHR does and they can be fine tuned to do it for you individually.
 So, I dove in head first. I looked at a number of systems. I demoed a number of systems. Two of my favorites took up an entire Saturday playing with them on my home computer. I quickly realized which one I liked after playing with the demo for an hour.
So, I dove in head first. I looked at a number of systems. I demoed a number of systems. Two of my favorites took up an entire Saturday playing with them on my home computer. I quickly realized which one I liked after playing with the demo for an hour.Colonoscopy Anyone?
I will warn you; however, selecting and implementing an electronic health record is like having a GI prep and colonoscopy without the sedation. It can be done, but it can be unpleasant.
It took an entire day to load the software on each of the workstations and server in my office. It took another 2-3 days to train my staff to use the software. It took us 2-3 months to realize that the computer will change the workflow drastically. (It took me a week to realize that there is nothing wrong with changing the workflow.) It took me a month to realize that you can practice medicine "outside the box." The workflow methodologies you learn in medical school and residency and establish in your office are malleable. And often your efficiency drastically improves when you accept this and then change them. There is a learning curve. When you accept this curve and stop fighting it, using your EHR becomes enjoyable.
What really makes it worth while is when all the parts of the puzzle fall into place. Lab interface, electronic prescribing, interoffice and inter-patient communication links allow streamlining of processes. You really can do today's work today.
(The first in a series of articles on EHR adoption, use, and integration)
Subscribe to:
Posts (Atom)